Did you get the message? My favorite behavior change studies can inform the COVID-19 response
April 11, 2020
By: Julia Rosenbaum, FHI 360
This article was originally posted on FHI 360’s R&E Search for Evidence Blog.

Photo credit: nopphonpattanasri/FreePik
Caught off-guard by the rapid novel coronavirus (COVID-19) transmission, governments and implementing partners are scrambling to develop prevention responses. To be effective, prevention communication must effectively spur individual and household actions. By now we’ve all seen the communication messages and know the recommended behaviors – for example, wash your hands frequently and at specific times, and don’t touch your face. But the question is: will current communications effectively trigger and sustain behavior change? I’ve been looking at behavior change evidence for many years, specifically in the context of handwashing. Success depends on how a message is crafted and how current evidence is applied. In this post, I explore some of my favorite evidence on fear-based messaging, the use of nudges to reflexively trigger behaviors, and specific determinants that influence handwashing behavior that I find useful. These studies can inform an evidence-based COVID-19 prevention and communication response.
Fear-based messaging alone doesn’t work to change behaviors
A common tactic to spur behavior change is the use of shock or fear. This tactic is too commonly used by health and communication professionals, government officials, and educators as well. But lessons learned from HIV prevention show that using fear tactics alone is ineffective, without a close link to a protective action and a high sense of efficacy to perform the action.
The Extended Parallel Process Model is a framework developed by Kim Witte (1992) to explain how individuals will react when exposed to fear messaging, considering both emotional and rational considerations as fundamental to the equation. Emotional factors include the individual’s perception of risk and severity of risk. The rationale sphere is perceived efficacy (Bandura, 1982) or one’s self-assessment of having the confidence, skills, social support and supplies to mitigate the risk. When fear is high, but efficacy is low, the individual will manage the fear – by minimizing the risk or ignoring the messaging – rather than managing the risk by taking protective action. When perceived efficacy to act is higher than fear, the individual will take the desired preventive actions.
The implications for COVID-19 prevention are clear. Avoid fear appeals, particularly without a close link to “small doable actions” that your target audience feels are feasible to take. If positive prevention actions are to be taken, the audience’s sense of efficacy must be greater than their fear. I developed figure 1 based on Witte’s model to illustrate the impact of fear-based messaging with and without efficacy and action. You can clearly see that fear messaging alone doesn’t change behaviors. With fear alone, people act to manage their fear, not the danger, in this case the danger of COVID-19.
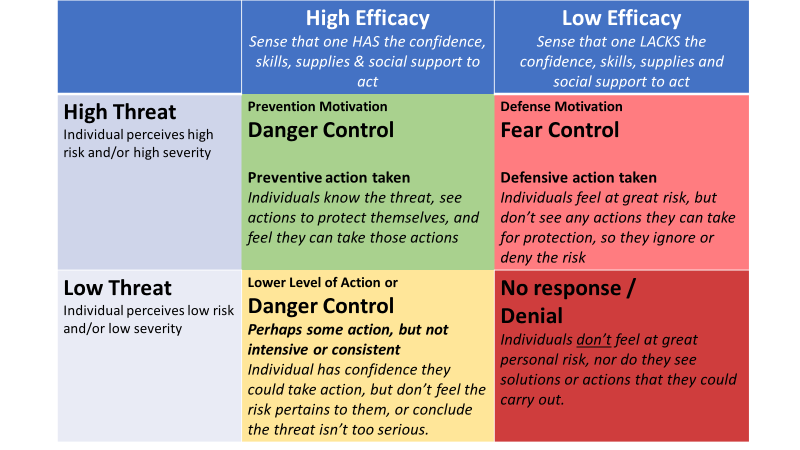
Figure 1: Developed based on Witte’s Extended Parallel Process Model (1992)
Incorporate reflexive cues or “nudges” into messaging
As I describe in a recent blog post, nudges are physical cues that influence individuals to behave in a certain way, without particular messaging or promotion of any behavior. Nudges avoid direct instruction, mandates or enforcement. The term “nudge” became popularized in 2008, after publication of Thaler and Sunstein’s book by that name. Nudges engage audiences at a subliminal level and work reflexively, rather than providing information to audiences to reflect upon and then act. An easy way to think of it: nudges are reflexive not reflective.
Nudge theory operates by designing elements or architecture in an environment which encourages positive or improved behaviors. Nudge principles have been applied for social good as well as in commercial marketing. For example, when searching for a hotel room on priceline.com, the pop-up saying “5 people are looking at this hotel right now!” nudges individuals to not lose the opportunity and book now! without actually promoting this action. Another example can be found at an airport or food court, where bakeries intentionally emit sweet cinnamon scents to spur you to buy donuts or cinnamon buns. Nudging has also been successfully used for traffic safety, recycling and toilet etiquette.
In what has now become the iconic handwashing nudge example, cheerful footsteps in demarcated pathways led Bangladeshi school children from school latrines to handwashing stations brightly decorated with handprints. Findings show these nudges to be an effective way to nudge children to wash their hands after the toilet. Without additional handwashing education or motivational messages, handwashing with soap among school children increased from 4% at baseline to 68% the day after nudges were completed – and 74% at both two-weeks and six-weeks post-intervention (Dreibelbis et al., 2016).

Photo credit: Dreibelbis et al., 2016; https://doi.org/10.3390/ijerph13010129
Findings show the nudge intervention and the hygiene education intervention to be equally effective at sustained impact over five months post-intervention (adjusted IRR 0.81, 95% CI 0.61-1.09). The simultaneous delivery of the hygiene education intervention significantly outperformed the sequential hygiene education delivery (adjusted IRR 1.58 CI 1.20-2.08), whereas no significant difference was observed between sequential and simultaneous nudge intervention delivery (adjusted IRR 0.75, 95% CI 0.48-1.17). These findings generated high interest in integrating nudges into behavior change programs; including, handwashing in health facilities (iNudgeyou, 2016), schools (Thrive Networks, 2017), and communities.A second, larger trial showed nudges to be as effective as intensive health education without the intensive or expensive effort (Grover et al., 2018). Researchers designed this study as a cluster-randomized trial, comparing rates of handwashing with soap after using the latrine (the primary outcome) between various intervention groups among primary school students in rural Bangladesh. Eligible schools were identified (government run with on-site sanitation and water, no hygiene interventions in the last year, and fewer than 450 students), and 20 randomly selected schools were then assigned to one of four interventions (with five schools per group): simultaneous handwashing infrastructure and nudges; sequential infrastructure then nudges; simultaneous high-intensity hygiene education and infrastructure; and sequential handwashing infrastructure and hygiene education.
Target the factors that most influence handwashing behavior change
Also essential for effective COVID-19 prevention communication is integrating what we know about relevant behavioral determinants. The final study included in this post is a bit of a cheat because it is a review of the literature (not findings from a single study) to identify the most influential determinants of handwashing behaviors in crisis and routine settings, synthesizing findings from 78 studies that met strict quality criteria. It’s hot off the presses, published after the emergence of COVID-19.
The review by White et al. concluded that our understanding of the determinants of handwashing “remains suboptimal” and found many limitations in how determinants are defined and measured. Unfortunately, the authors are not able to draw solid conclusions about the determinants of behavior in outbreaks or crisis. They did more generally identify the most commonly reported determinants: risk, psychological trade-offs or discounts, knowledge, demographic (non-behavioral) traits (like gender, wealth and education), and infrastructure. The authors conclude, “Hygiene promotion programmes are likely to be most successful if they use multi-modal approaches, combining infrastructural improvement with ‘soft’ hygiene promotion which addresses a range of determinants rather than just education about disease transmission.”
In conclusion, even though the situation with COVID-19 feels new, it turns out we have a lot of existing evidence from handwashing promotion that’s highly relevant to inform prevention interventions. Applying the findings from these studies sets you on the road to effective COVID-19 prevention and communication efforts. Nudges work to influence behavior; I encourage you to develop and test nudges for prevention behaviors like physical distancing! Also, fear doesn’t trigger protective behaviors, but assuring individuals have the skills, supplies, social support and efficacy to carry out feasible behaviors will make it more likely that they try and maintain preventive practices. And build in the evidence on determinants into your planning of COVID-19 behavior change activities.